CCCS Internal
CCCS Internal SP 19-40b – Emergency Operations and Management Planning
Colorado Community College System / System Procedure
SP 19-40b
APPROVED: March 27, 2015
EFFECTIVE: March 27, 2015
REVISED: March 10, 2021
REVISED: February 8, 2023
REVISED: September 13, 2023
REVISED: December 13, 2023
APPENDIX REVISED: December 13, 2023
REFERENCE(S): Board Policy (BP) 19-40, Emergency and Safety Planning; Colorado Revised Statutes (C.R.S.) § 23-5-149, §§ 25-47-101 et seq.
APPROVED:
/ Joseph Garcia /
Joseph A. Garcia, Chancellor
APPLICATION
This procedure applies to the Colorado Community College System, including its Colleges (CCCS or System).
BASIS
In accordance with Board Policy (BP) 19-40, Emergency and Safety Planning, the Colleges and the System Office must adopt and implement a written Emergency Operations Plan (EOP) to address specific hazards and circumstances that constitute an emergency for staff, faculty, students, and property, and shall implement safety measures as approved by the Chancellor or as required by law.
PROCEDURE
EOP Requirements:
Each College and the System Office must:
- Implement and keep their EOP current.
- Ensure the EOP serves as a guide for emergency management and shall coordinate all phases of emergency response in order to minimize the impacts of disasters and incidents, to protect people and property, and to restore any interruptions to CCCS operations.
- Review and update their EOP at least annually.
Additional Safety Measure Requirements:
- Each College and the System Office must conduct regular training exercises as part of their emergency response preparations.
- Each College and the System Office must conduct annual active shooter and bleeding control trainings (e.g., STOP THE BLEED training).
- Should an exceptional circumstance exist that prevents a College or the System Office from meeting these training requirements, the President or Director of Emergency Management must seek approval from the Chancellor.
- Each College and the System Office must have bleeding control kits (e.g., STOP THE BLEED kits) on site, in conspicuous areas.
- Each College is required to acquire and stock a supply of Epinephrine Auto-Injectors (Epi Pens) and:
- Colleges are encouraged to place them in reasonable quantities to ensure there is availability for use by any person perceived to be experiencing anaphylaxis.
- The placement of Epi Pens should focus on areas where students gather in the largest volumes such as, but not limited to, residence halls and dining areas.
- Colleges are required to make the location of the Epi Pens publicly known.
- In order to obtain a supply of Epi Pens, Colleges are allowed to accept donations, gifts, grants, including in-kind donations, or purchase directly from a healthcare provider.
- Colleges are required to designate an employee(s) to complete an anaphylaxis training program conducted by a nationally recognized organization experienced in training laypersons in emergency health treatment or by an individual or entity approved by the Colorado Department of Health and Environment (CDPHE).
- Training will be a conditional requirement for a health-care practitioner to direct a distribution of Epi Pens from an in-state prescription drug outlet to the College.
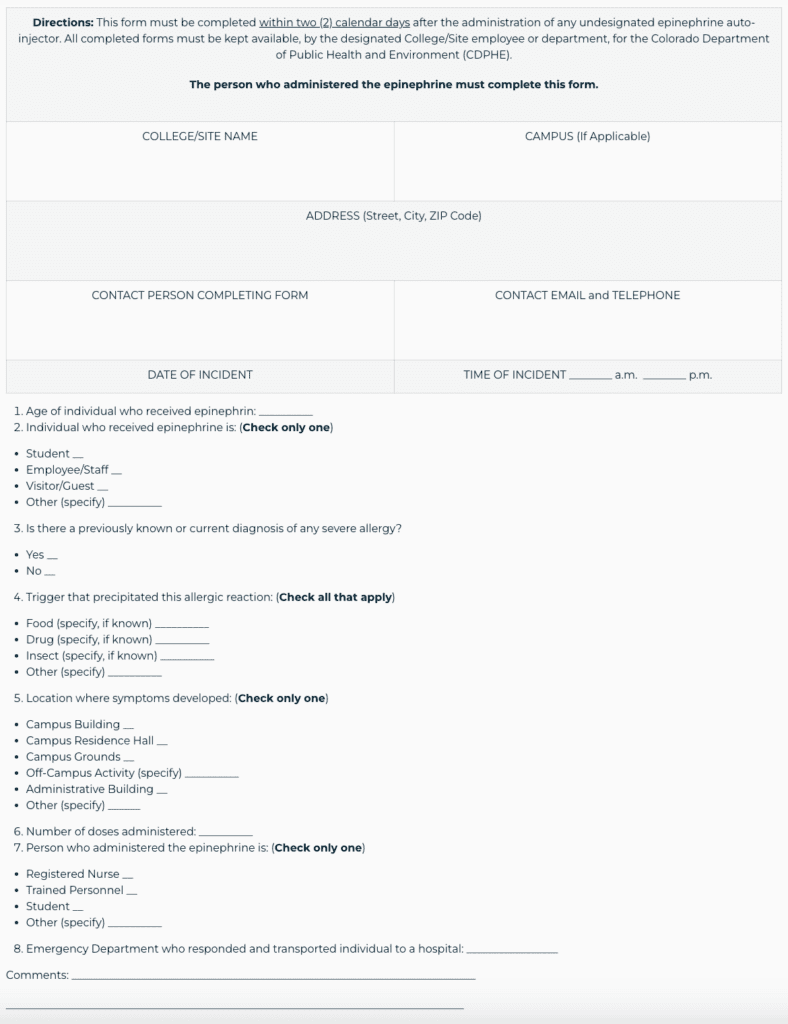
- Each College must keep a report of each incident whereby an Epi Pen was used on their premises and have the report available if requested by CDPHE.
- See Appendix A for the Reporting form.
REVISING THIS PROCEDURE
CCCS reserves the right to change any provision or requirement of this procedure at any time and the change shall become effective immediately.
APPENDIX A
Undesignated Epinephrine Reporting Form